The latest estimates of under-5 mortality from the UN Inter-agency Group for Child Mortality Estimation (IGME) show a one-third decline at the global level of under-5 mortality rates from 89 deaths per 1000 livebirths in 1990 to 60 in 2009. Over the same period, the total number of under-5 deaths has decreased from 12·4 million in 1990 to 8·1 million in 2009. This is further evidence that progress on child mortality is being made across all regions of the world, with many regions having reduced the under-5 mortality rate by 50% or more. With only 5 years left until the 2015 deadline to achieve the Millennium Development Goals (MDGs), world leaders will gather in New York for the High Level Plenary Meeting on MDGs on Sept 20–22 with the aim of accelerating progress. These IGME estimates are the latest available information on child mortality to provide a basis for assessing progress and reaching consensus for action.
| Region | 1990 | 1995 | 2000 | 2005 | 2007 | 2008 | 2009 | Decline 1990–2009 (%) | Average annual rate of reduction 1990–2009 (%) | Progress towards MDG 4 target * | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Developing regions | 99 | 95 | 84 | 74 | 70 | 68 | 66 | 33 | 2·1 | Insufficient | |
| Northern Africa | 80 | 60 | 46 | 33 | 30 | 28 | 26 | 68 | 5·9 | On track | |
| Sub-Saharan Africa | 180 | 175 | 160 | 143 | 136 | 133 | 129 | 28 | 1·8 | Insufficient | |
| Latin America and the Caribbean | 52 | 43 | 33 | 27 | 24 | 23 | 23 | 56 | 4·3 | On track | |
| Eastern Asia | 45 | 44 | 36 | 25 | 22 | 20 | 19 | 58 | 4·5 | On track | |
| Eastern Asia (excluding China) | 28 | 36 | 29 | 18 | 18 | 17 | 17 | 39 | 2·6 | On track | |
| Southern Asia | 122 | 110 | 95 | 79 | 74 | 72 | 69 | 43 | 3·0 | Insufficient | |
| Southern Asia (excluding India) | 131 | 118 | 101 | 86 | 81 | 80 | 78 | 40 | 2·7 | Insufficient | |
| South-eastern Asia | 73 | 58 | 48 | 41 | 39 | 37 | 36 | 51 | 3·7 | On track | |
| Western Asia | 66 | 56 | 44 | 36 | 33 | 32 | 31 | 53 | 4·0 | On track | |
| Oceania | 76 | 69 | 65 | 62 | 60 | 60 | 59 | 22 | 1·3 | Insufficient | |
| Countries of the Commonwealth of Independent States (CIS) | 46 | 48 | 39 | 29 | 26 | 25 | 23 | 50 | 3·6 | On track | |
| CIS in Europe | 26 | 25 | 23 | 17 | 15 | 14 | 13 | 50 | 3·6 | On track | |
| CIS in Asia | 78 | 73 | 62 | 47 | 42 | 39 | 37 | 53 | 3·9 | On track | |
| Developed regions | 12 | 9 | 8 | 7 | 6 | 6 | 6 | 50 | 3·6 | On track | |
| Transition countries of south-eastern Europe | 31 | 25 | 20 | 15 | 13 | 12 | 11 | 65 | 5·5 | On track | |
| World | 89 | 86 | 77 | 67 | 63 | 62 | 60 | 33 | 2·1 | Insufficient | |
The IGME was established in 2004 to improve monitoring of progress towards achievement of MDG 4, and to enhance the capacity of countries to produce timely estimates of child mortality. It is led by UNICEF and WHO, and also includes the UN Population Division and the World Bank. The group is advised by an independent Technical Advisory Group of leading experts in areas of demography and biostatistics.
The IGME compiles all available nationally-representative data on child mortality. Civil registration systems are the preferred source of data on child mortality because they collect information as events occur and cover the entire population. However, many developing countries lack fully functioning systems for civil registration that accurately record all births and deaths. Therefore national household surveys are the primary source of data on child mortality for most developing countries. Country-specific estimates are obtained from a regression line fitted to all observations that meet the quality standards established by the IGME, and extrapolated to a common reference year (2009; description of methods in webappendix).
New data, for 40 developing countries, have been incorporated since derivation of the 2008 estimates.
These data have resulted in substantial changes in estimates of child mortality for some countries. Because the regression line is based on the entire time series of data for each country, estimates presented here might differ from and not be comparable with previous estimates. The latest country-specific estimates and underlying data sources are in 1 and 4, respectively.
In the developing world, northern Africa and eastern Asia have made the greatest progress in reducing under-5 mortality (by 68% and 58% respectively) between 1990 and 2009. At country level, among countries with an under-5 mortality rate above 40 per 1000 livebirths, ten countries reduced their rate by at least half.
Of these Bangladesh, Eritrea, Laos, Madagascar, Nepal, and Timor-Leste recorded at least a 60% decline. In absolute terms, the greatest reductions in the under-5 mortality rate since 1990 have been achieved by Ethiopia, Liberia, Madagascar, Malawi, Niger, and Timor-Leste (surpassing 100 points during the period). Overall the number of countries with under-5 mortality of 100 deaths per 1000 livebirths or higher declined from 52 in 1990 to 31 in 2009. Moreover, the rate of decline in under-5 mortality has doubled from 1·4% per year in the 1990s to 2·8% in 2000–09.
The highest rates of mortality in children under age 5 years continue to occur in sub-Saharan Africa where, in 2009, one in every eight children (129 per 1000 livebirths) died before their fifth birthday—a level nearly double the average in developing regions (66 per 1000) and around 20 times the average for developed regions (6 per 1000). All the 31 countries with under-5 mortality exceeding 100 per 1000 livebirths in 2009, except Afghanistan, are in sub-Saharan Africa. However, there are encouraging findings from this region. Four of the ten countries with more than a 50% reduction in under-5 mortality between 1990 and 2009 are located in sub-Saharan Africa. Furthermore, five of the six countries with a reduction of more than 100 deaths per 1000 livebirths are in this region.
Under-5 mortality is increasingly concentrated: 70% of the world’s under-5 deaths in 2009 occurred in only 15 countries. About half of the deaths occurred in only five countries: India, Nigeria, Democratic Republic of the Congo, Pakistan, and China. India and Nigeria together account for nearly one-third of the total number of under-5 deaths worldwide (21% and 10%, respectively).
A common feature of countries that have made the most substantial progress, especially in sub-Saharan Africa, has been rapid expansion of basic public health and nutrition interventions, such as immunisation, breastfeeding, vitamin A supplementation, and safe drinking water. However, on the whole, coverage of low-cost curative interventions against pneumonia, diarrhoea, and malaria, which together cause over half the under-5 deaths in the region, remains low.
These interventions need to be expanded. In southern Asia, more than half of all childhood deaths occur in the first 28 days after birth. To substantially reduce these deaths, innovative solutions, such as the Janani Suraksha Yojana programme in India (which provides compensation for women to deliver in designated centres) or the increasing use of public–private partnerships to improve provision of skilled delivery services, are required. Undernutrition is an underlying cause of at least a third of all under-5 deaths. Reducing both chronic and acute undernutrition will have a substantial impact on reducing child mortality. Furthermore, improved coverage of specific nutrition interventions, such as early and exclusive breastfeeding, will reduce the prevalence of pneumonia and diarrhoea, which are the main causes of child deaths. If progress in child mortality reduction is to be sustained and accelerated, continued investments and innovation will be required, especially in the three regions that are not currently on track to achieve MDG 4: sub-Saharan Africa, southern Asia, and Oceania.
Overall progress masks inequalities within countries. Gender discrimination and low levels of education remain powerful determinants of inequities. Across China and India, for example, girls have a higher under-5 mortality than boys—the reverse of the situation in most other countries. The children of educated mothers are more likely to survive than children of mothers with no education. The largest ratio between these two groups occurs in Latin America and the Caribbean, where the difference is more than three-fold.
Although data are available for only a limited number of countries (38), more countries increased relative disparity between poor and rich over the last two decades than decreased it, with twice the number of countries in the upper left quadrant of the figure compared to those in the lower left quadrant of the figure. The inference is that, even though national under-5 mortality has been reduced in many countries, disparity between poor and rich has generally increased. Removing financial and social barriers to accessing welfare services, innovations to make supply of critical services more available to the poor, and increasing local accountability of the health systems are examples of policy interventions that have allowed health systems to improve equity.
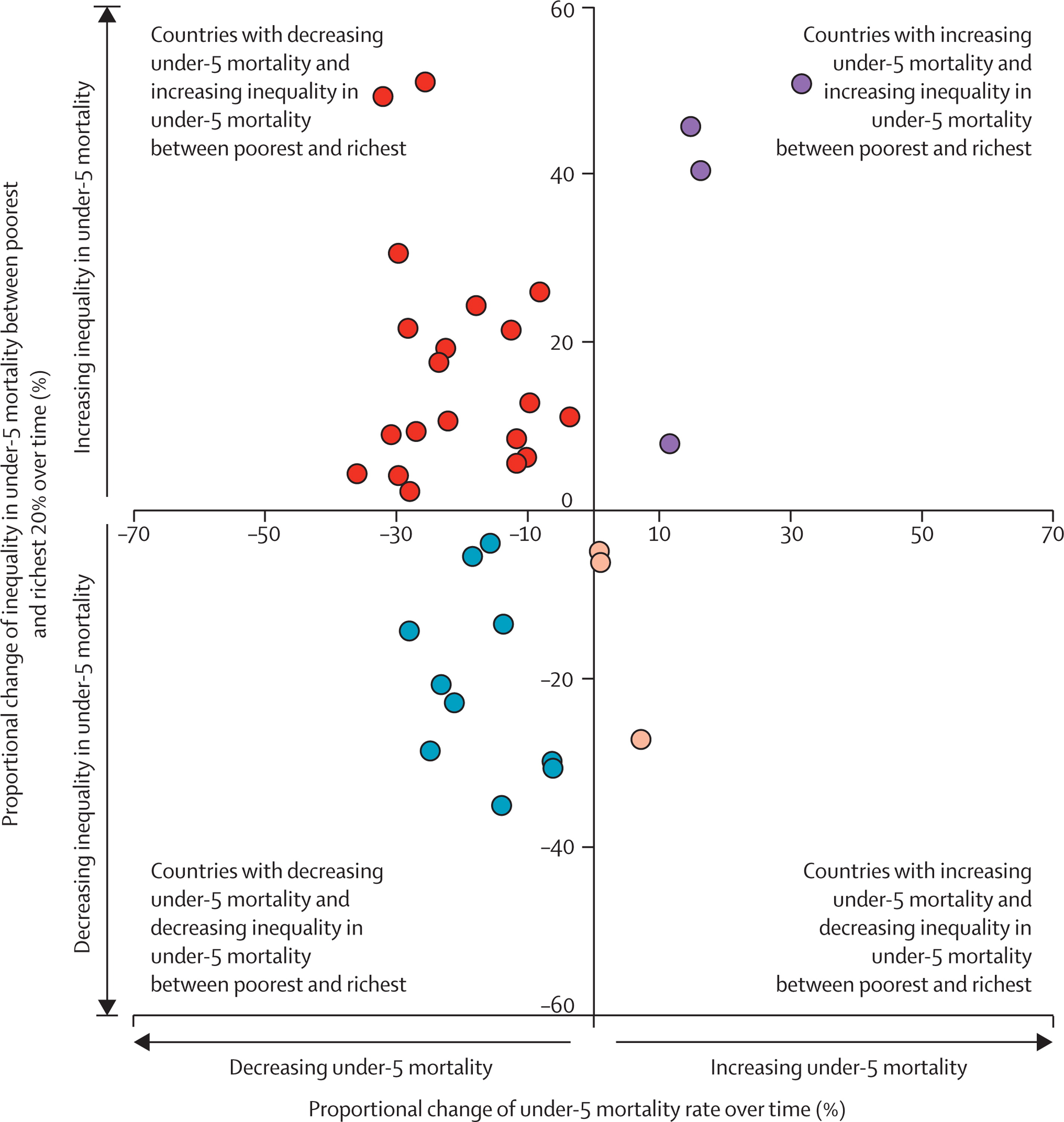
From subset of 38 countries with available data. 18 countries among 26 countries with 10% or more decrease in under-5 mortality had increasing or stagnant inequality in under-5 mortality between poorest 20% and richest 20%. Of these 18 countries, ten increased inequality in under-5 mortality by 10% or more.